Malawi Priorities: Malaria
Technical Report
Key Messages
- Although malaria is a largely preventable and treatable disease, it is a significant cause of mortality, morbidity, and productivity loss in Malawi. This study estimates that in 2019, malaria generated health and productivity losses equivalent to MWK 94,770 million – or 1.7 percent of GDP. Increasing insecticide resistance and less than optimal (60%) care-seeking behavior represent two of the most pressing issues facing the country when it comes to reducing the burden of malaria.
- The main policy recommendation from this cost-benefit analysis is that the National Malaria Control Program (NMCP) should fully adopt piperonyl butoxide (PBO) insecticide-treated bednets (ITNs) and rollout community-informed mass media to increase the rate at which people seek formal care when they, or their children, have a fever. PBO ITNs have been shown to have greater effectiveness against mosquitos compared to the ITNs that Malawi has used in the past.
- From 2021 to 2030, these interventions would require an additional MWK 46,000 million, or USD 62m investment, representing an ~ 8 percent increase in the malaria budget. This would reduce expected malaria deaths by 18,129 (a 45% reduction) and expected cases of malaria by 10.4 million (a 25% reduction) over 10 years. The benefit-cost ratio (BCR) is 6.6 meaning that for every kwacha invested in these interventions the social and economic return is 6.6 kwacha.
- This return would be even larger (BCR = 13.2) if insecticide resistance becomes twice as strong as assumed in the analysis, a reasonable possibility in Malawi.
- The study identifies two potential interventions which are likely to be less cost-effective: scaling up indoor residual spraying (IRS) in districts near Lake Malawi and reducing the frequency of ITN mass campaigns from every 3 years to every 2 years. We suggest more careful consideration and analysis of these two interventions, ideally with additional years of pilot field data, before institutionalizing these policy changes.
Context
Although Malaria is a largely preventable and treatable disease, it is a significant cause of mortality, morbidity, and productivity loss in Malawi. With around 15% of the population suffering from the disease in Malawi at any given point in time, it creates a large burden on the health system, accounting for 36 percent of all outpatient visits and 15 percent of all hospitalizations. This study estimates that in 2019, malaria generated welfare losses equivalent to MWK 94,770 million – or 1.7 percent of GDP – when considering mortality, cost of illness, lost productivity, and lost learning.
Over the years, the number of malaria cases has been showing a declining trend in Malawi. The Malawi NMCP has been quite efficient - investing significantly in vector control, prevention in pregnancy, testing, and case management. Traditionally high BCR interventions are likely already implemented. The continual ITN distribution program which provides around one million long-lasting ITNs during antenatal care (ANC) and child immunization visits have also helped, supplemented by periodic mass distribution campaigns that provide more general coverage. Malawi has also rolled out intermittent preventative treatment for malaria during pregnancy (IPTp) in ANC (which as the literature suggests is a high BCR intervention), with a substantial proportion (78 percent) of pregnant women receiving at least two doses of IPTp. In terms of testing and case management, since 2018 more than 98 percent of fever cases who present at health facilities are tested for malaria, and of those infected, close to 100 percent receive ACT-based first-line treatment.
While the approach and focus on reducing the malaria burden are commendable, several challenges remain which, if unaddressed, could retard or even reverse the significant progress made thus far. These include:
- Emerging insecticide resistance particularly to pyrethroid leading to reduced ITN effectiveness.1
- Suggestive evidence is that a significant amount of ITNs in Malawi only last for two years in practice, leaving many people unprotected in the year before each triennial mass distribution campaign.
- While testing is near-universal, only ~ 60 percent of people, or parents of children, seek care for fever (NSO, MDHS, 2015-2016) – meaning that a considerable proportion of malaria cases are not diagnosed and treated. This large number of undiagnosed and untreated cases substantially adds to the population-level burden of malaria morbidity, mortality, transmission, and economic losses.
This paper focuses on cost-benefit analyses of interventions using the Spectrum-Malaria epidemiological projection model2 for determining their impact.
Combining PBO nets with mass media to boost care-seeking for fever has the highest return on investment
NMCP distributes approximately one million ITNs every year during routine ANC and immunization, and almost 11 million ITNs every 3 years as part of the mass distribution campaign for the general population. While in the past the distribution has consisted mostly of pyrethroid-only ITNs, the paper recommends a complete switch to PBO nets distribution instead to address growing insecticide resistance.
The paper also recommends the rollout of a mass media intervention for improved care-seeking for fever. This would require the first year of community dialogues to design context-specific messages (across 10,000 people in 28 districts). Then from the second half of the first year, dissemination via radio messaging would craft a mass media promotion (radio) specific to each district. This is expected to increase fever care seeking by 10pp from 60 to 70 pp
Figure 1: Timeline of costs and benefits of Community-informed mass media + PBO ITN
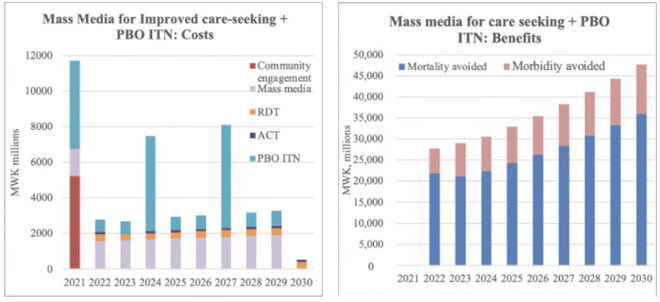
The cost drivers for these interventions would include the extra investment on PBO nets which cost MWK 462 more than the standard pyrethroid ITN. With 11m ITNs being distributed every three years and 1m in the years in between, this would cost an additional MWK 20,729 million.
Costing mass media for improved care-seeking for fever, we assume an initial message design cost for community dialogues aimed at 10,000 people in each of the 28 districts. The community dialogues would cost MWK 18,625 per person,3 while the mass media component would cost MWK 75 per capita.4 This intervention furthermore changes the usage of RDT and ACT, due to increased care-seeking. The cost of RDT is set at MWK 335,5 while the cost of a course of first-line ACT is MWK 2,235.6 The total additional investment over 10 years would be MWK 24,718 million.
The study recommends transitioning to 100 percent PBO ITN distribution along with a community-informed mass media rollout for improved care-seeking for fever. The combined intervention would require an additional MWK 46,000 million over a 10-year period, or USD 62m, representing ~ 8 percent of the expected budget of an annual USD 80 million.7 The time series of costs is presented in the figure below. This intervention has the largest absolute effect of all interventions considered, avoiding expected malaria deaths by 18,129 (a 45% reduction) and expected cases of malaria by 10.4 million (a 25% reduction) from 2022-2030.
Overall, the analysis indicates that PBO ITNs and mass media for improving fever care-seeking are likely the most efficient use of additional resources for the NMCP. The combination of the two interventions would bring Malawi closer to its malaria targets.
In contrast, IRS in the districts around Lake Malawi as well as increasing the frequency of mass ITN distribution campaigns are a likely less effective use of resources. For further details on these calculations please consult the accompanying technical report.
Summary Table
| Intervention | BCR | Beneficiary Group | Extra Costs over a 10-year period | Extra Benefits over a 10-year period | Cost per Death Avoided |
|---|---|---|---|---|---|
| Mass media for improved care seeking for fever | 7.4 Good | All Malawians | MWK 24,718 million | 12,312 deaths and 4.9m cases avoided | MWK 2.0m |
| 100 percent PBO ITN distribution | 6.0 Good | 10.7 million households | MWK 20,729 million | 6,767 deaths and 6.1m cases avoided | MWK 3.1m |
| Mass media for improved care seeking for fever + 100 percent PBO ITN distribution | 6.6 Good | All Malawians | MWK 46,000 million | 18,129 deaths and 10.4m cases avoided | MWK 2.5m |
| Scale-up IRS in districts around Lake Malawi | 1.7 Fair | 2.1 million people in districts around Lake Malawi | MWK 5,827 million | 507 deaths and 0.4m cases avoided | MWK 11.5m |
| Increasing frequency of mass ITN campaigns from once every 3 years to once every 2 (PBO or pyrethroid-only) | <1 Poor | All Malawians | 40% extra costs | Only 20% increase in benefit over a 6-year period |
Note: BCRs are based on costs and benefits discounted at 8% (see accompanying technical report). BCR ratings are determined on the following scale Excellent, BCR > 15; Good, BCR 5-15; Fair, BCR 1-5; Poor, BCR < 1. This traffic light scale was developed by an Eminent Panel including several Nobel Laureate economists for a previous Copenhagen Consensus project that assessed the Sustainable Development Goals.
Download the full policy brief here.